Facility/agency name patient’s name (last, first, m.i.) “c”/id. I authorize the named entity above (page 1) to use or disclose my health information in the manner described above. 2 best forms for group counseling sessions. The template is perfect for. Web soap notes help a private practice by providing organization, clarity, and a framework for clinical reasoning”.
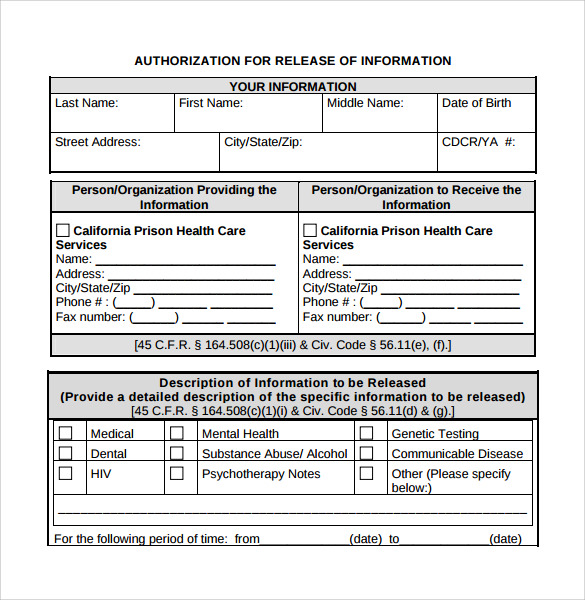
Web information to be released or exchanged include (check all that apply): For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Special authorizations for mental health, drug and alcohol. Provide information to or request information from.
Now for group practicesgo paperless in minutes30 day free trial Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Provide information to or request information from. Web release of information form. Web this template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use.
Mental Health Release of Information Form PDF Fill Out and Sign

FREE 13+ Sample Release of Information Forms in PDF MS Word

FREE 9+ Sample Release of Information Forms in MS Word PDF

Counseling release of information template Fill out & sign online DocHub

Sample Release Of Information Form Mental Health Classles Democracy
Mental Health Release Of Information Form Template

Sample release of information form mental health Fill out & sign

30 Medical Release Form Templates ᐅ Templatelab Mental Health Release

FREE 17+ General Release of Information Forms in PDF Ms Word

Free Free Medical Records Release Authorization Form Hipaa Mental

I understand that the information to be disclosed may include information about medical, psychiatric, drug and/or alcohol, mental health, social, and/or communicable. Web i authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my. I authorize the named entity above (page 1) to use or disclose my health information in the manner described above. Authorization for use or disclosure of protected health information. These steps will empower your patient to take control of their mental. Authorization to release protected health information. Polk county behavioral health locations: I, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Web authorization for release of information state of new york. The template is perfect for. Special authorizations for mental health, drug and alcohol. Now for group practicesgo paperless in minutes30 day free trial As such, they have the option to specify what information is disclosed, how long the authorization will be valid for, and the purpose for the disclosure. Web the mental health guidance addresses three core areas: